
Central Venous Oxygen Saturation and Central Venous Pressure in Cardiogenic Shock
- Faraz Afzal
- Feb 8
- 13 min read

A Practical, Physiology-Based Guide for Clinical Decision-Making
In cardiogenic shock and advanced heart failure, due to practical reasons, treatment often has to be guided without access to advanced invasive hemodynamic monitoring. In everyday clinical practice, central venous oxygen saturation (SvO₂/ScvO₂) and central venous pressure (CVP) (apart from echocardiography and arterial line) are among the most readily available and frequently used clinical tools and parameters.
This article provides a physiologically grounded review of how SvO₂ and CVP can be used - and misused - to assess cardiac output, congestion, and treatment response in cardiogenic shock, with lactate as a necessary corrective marker.
Introduction – Why This Article Is Necessary
Cardiogenic shock is one of the most complex and lethal conditions in acute medicine and cardiology. Despite this, management in most real-world settings must be performed without pulmonary artery catheters or advanced invasive monitoring.
Clinical decisions are therefore often based on parameters derived from a central venous catheter, primarily:
Central venous oxygen saturation (SvO₂ / ScvO₂)
Central venous pressure (CVP)
Lactate
This article offers a physiology-driven framework for understanding what these variables actually represent, their limitations, and how they should be integrated in patients with cardiogenic shock and severe heart failure.
What Is Cardiogenic Shock? (Brief Review)
Cardiogenic shock can be defined as:
Inadequate organ perfusion secondary to cardiac dysfunction.
Key characteristics include:
Low cardiac output
Compensatory systemic vasoconstriction
Rising cardiac filling pressures
Tissue hypoperfusion and progressive organ failure
The fundamental principle is:
Cardiogenic shock is a low-flow shock - not primarily a low-pressure shock.
Blood pressure may appear preserved, while tissue and organ perfusion are critically impaired.
Clarification Regarding Echocardiography
In addition to parameters from a central venous catheter and arterial line, cchocardiography is a central component of the assessment of cardiogenic shock and can provide decisive information regarding both underlying mechanism and hemodynamics. With adequate acoustic windows, accurate measurement of the left ventricular outflow tract (LVOT), and a representative LVOT velocity–time integral (VTI) signal, cardiac output can be reliably estimated and actively used to guide therapy
.
This article is, however, deliberately focused on the use of central venous oxygen saturation (SvO₂/ScvO₂) and central venous pressure (CVP), as these parameters are often continuously available and provide practical bedside decision support in everyday clinical practice. This focus does not imply that CVP and SvO₂ are sufficient in isolation, but rather that they represent part of a comprehensive assessment, in which clinical findings, echocardiography, laboratory parameters, and response to treatment must always be integrated.
Oxygen Delivery and Demand: What Central Venous Oxygen Saturation (SvO₂) Really Measures
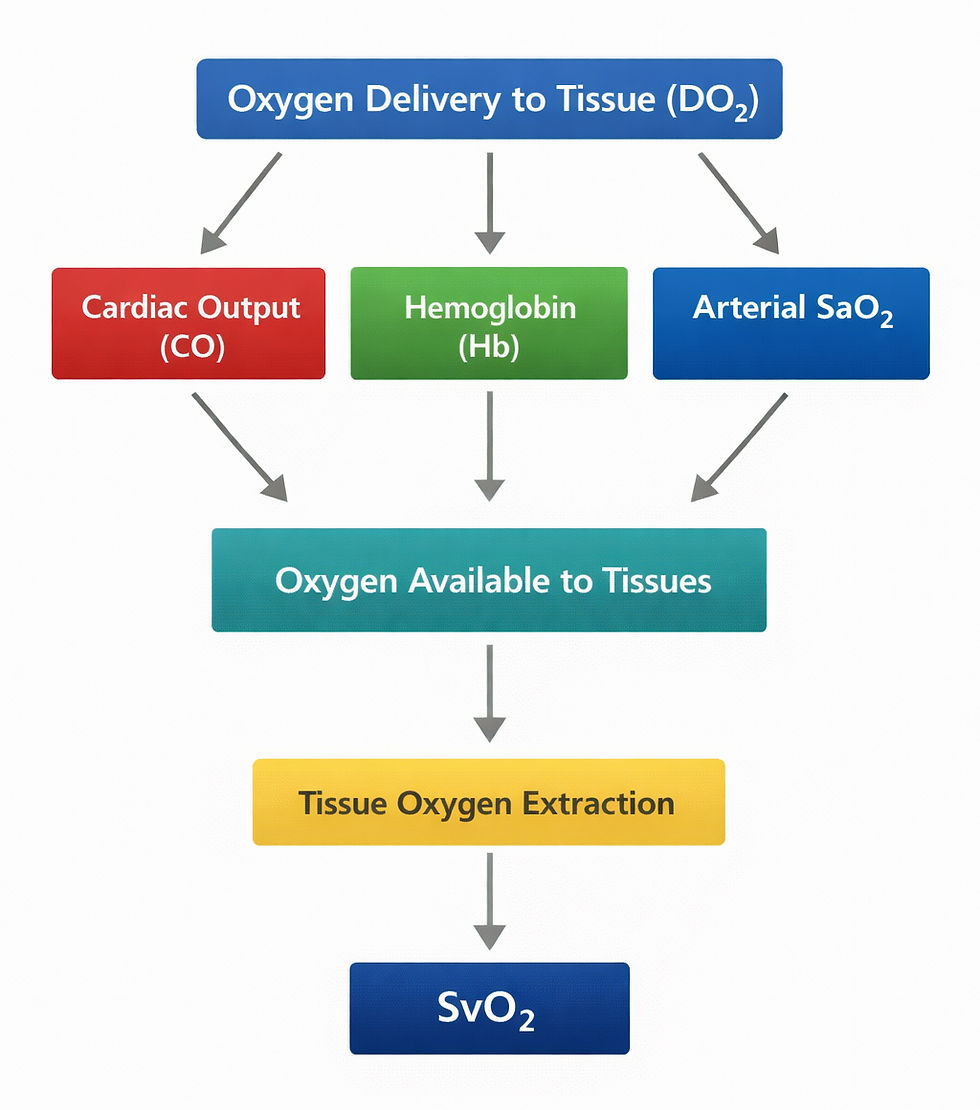
All hemodynamic assessment in shock can essentially be reduced to the balance between oxygen delivery (DO2) and oxygen consumption (VO2) in peripheral tissues.
Total tissue oxygen delivery is determined by three factors:
Cardiac output (CO)
Hemoglobin concentration (Hb)
Arterial oxygen saturation (SaO2)
In cardiogenic shock, the primary problem is usually insufficient cardiac output, which reduces oxygen delivery to the tissues. When oxygen delivery fails to meet metabolic demand, tissues compensate by increasing oxygen extraction. As a result, less oxygen is returned to the venous circulation.
This is the physiological basis for the use of central venous oxygen saturation (SvO2).
When measured via a central venous catheter, ScvO₂ primarily reflects venous blood from the upper body. ScvO₂ provides information about the balance between oxygen delivery and oxygen consumption and can be used as a real-time surrogate for global flow when the necessary assumptions are met.
A low SvO₂ indicates increased oxygen extraction and inadequate oxygen delivery, most commonly due to low cardiac output.
A rising SvO₂ generally suggests an improved balance between oxygen supply and demand and may reflect an improvement in flow.
It is, however, important to recognize that a normal or increasing SvO₂ does not necessarily indicate clinical improvement. In advanced shock states, whether septic or cardiogenic, tissue oxygen extraction may be impaired (cytopathic hypoxia), resulting in a falsely elevated SvO₂ despite ongoing tissue hypoxia. In such situations, this discrepancy is typically reflected in the clinical picture and in other perfusion markers, particularly lactate.
Nevertheless, in cardiogenic shock, SvO₂ remains the most important continuous real-time parameter for assessing changes in cardiac output in clinical practice, provided that it is always interpreted in conjunction with clinical findings and other available data.
ScvO2 (Central Venous Catheter) versus Mixed SvO2 (Pulmonary Artery)
It is important to distinguish between central venous oxygen saturation measured via a central venous catheter (ScvO2) and true mixed venous oxygen saturation (SvO2) measured in the pulmonary artery.
Mixed SvO2 obtained from the pulmonary artery represents a mixture of venous blood from both the upper and lower body (via the superior and inferior vena cava), and therefore provides the most comprehensive assessment of global oxygen balance. However, this requires a pulmonary artery catheter, which is not routinely available in most clinical settings.
ScvO2 measured via a central venous catheter primarily reflects oxygen saturation in venous blood from the upper body. Under hemodynamically stable conditions, ScvO2 and mixed SvO2 may be relatively similar. In shock states, particularly in cardiogenic shock, they can diverge substantially.
This divergence occurs because tissue perfusion and oxygen extraction are often unevenly distributed during shock. Splanchnic organs and the lower extremities may be severely hypoperfused, while the brain and upper body are preferentially perfused. As a result, ScvO2 may overestimate global oxygen balance.
Despite these limitations, ScvO2 has substantial clinical value because it is readily available, reproducible, and well suited for trend monitoring. When interpreted correctly, changes in ScvO2 often provide more clinically relevant information than isolated measurements of mixed SvO2, particularly when assessing response to therapeutic interventions.
The key issue is therefore not whether SvO2 is “true” mixed or central venous, but whether the clinician understands the limitations and uses the measurement consistently as a trend within the clinical context.
A Critical Prerequisite: Stable Hb and SaO2
SvO2 is not a direct measure of cardiac output, but rather an expression of the balance between oxygen delivery and oxygen consumption. If any component of oxygen delivery changes, SvO2 will change as well—independently of cardiac output.
If:
Hemoglobin concentration decreases, or
Arterial oxygen saturation (SaO2) is reduced,
total oxygen delivery to the tissues will fall even if cardiac output remains unchanged. Tissues will then increase oxygen extraction, leading to a decrease in SvO2. If Hb and SaO2 are not assessed simultaneously, this may be misinterpreted as reduced flow.
Conversely, SvO2 may increase with higher SaO2 or reduced oxygen consumption without any true improvement in cardiac output.
SvO2 can therefore only be interpreted as a meaningful surrogate for flow when hemoglobin concentration, arterial oxygen saturation, and oxygen consumption are relatively stable.
Clinical Rule of Thumb
SvO2 reflects global oxygen balance, not cardiac output in isolation. Changes in hemoglobin, SaO2, or oxygen consumption will alter SvO2 - even in the absence of any change in flow.
Central Venous Pressure (CVP)
What CVP Is - and What It Is Not
CVP reflects right atrial pressure and represents:
Right-sided filling pressure
Venous return
The interaction between volume, compliance, and cardiac pump function
CVP is not a direct measure of intravascular volume.
In heart failure, an elevated CVP most often indicates:
Venous congestion
Reduced ventricular compliance
Unfavorable filling conditions
Why CVP Matters Clinically
CVP directly affects organ perfusion:
Perfusion pressure ≈ MAP − CVP
As CVP rises, effective perfusion of the kidneys, liver, and gut decreases—even when mean arterial pressure appears acceptable.
An isolated rise in CVP without improvement in flow indicates that the heart is not preload-responsive. Additional filling is converted into congestion rather than increased stroke volume, leading to:
Worsening organ perfusion
Deteriorating hemodynamics
This is a central clinical insight in cardiogenic shock management. An ScvO₂ < 60% is associated with an increased risk of major cardiovascular events and a poorer prognosis in patients with acute decompensated heart failure and cardiogenic shock.
Key Parameters at a Glance
Parameter | Normal Range | Concerning Value | Clinical Interpretation |
ScvO₂ | 65–75% | <60% | Suggests low cardiac output if Hb, SaO₂, VO₂ are stable |
CVP | 2–6 mmHg | >10–12 mmHg | Indicates congestion, not volume status |
CVP ≥15 mmHg | – | High risk | Organ hypoperfusion likely |
When CVP Can Be Misleading – Clinical Limitations
Central venous pressure (CVP) reflects the pressure in the right atrium and serves as a marker of right-sided filling pressure and venous congestion. Under normal conditions, CVP can provide useful information about venous return and cardiac filling pressures. In a number of clinical conditions, however, the relationship between CVP, preload, and fluid responsiveness breaks down. In these situations, CVP primarily represents pressure load rather than functional filling, and may therefore provide a misleading basis for clinical decision-making.
A common feature of these conditions is an increase in right atrial pressure without a corresponding increase in effective forward flow.
Isolated Right Ventricular Failure
In isolated right ventricular failure, CVP is often elevated due to impaired forward pumping function of the right ventricle. The elevated CVP reflects reduced emptying of the right atrium, and not necessarily increased intravascular volume. In this setting, a high CVP may coexist with low left ventricular preload, and additional fluid administration will often worsen right ventricular dilation and reduce left ventricular filling through ventricular interdependence.
Ventricular interdependence refers to the phenomenon whereby overfilling or dilation of the right ventricle impairs left ventricular filling and function.
Significant Tricuspid Regurgitation
In moderate to severe tricuspid regurgitation, CVP is strongly influenced by regurgitant flow from the right ventricle into the right atrium. CVP may therefore become markedly elevated without any meaningful relationship to preload or volume status, and changes in CVP following fluid administration or diuretic therapy are difficult to interpret. In practice, CVP loses its role as a guiding parameter and should primarily be regarded as an indicator increased regurgitation volum resulting in increased pressure in the right atrium.
Portal Hypertension, Ascites, and Increased Intra-abdominal Pressure
In portal hypertension and significant ascites, increased intra-abdominal pressure and reduced venous compliance within the splanchnic circulation may lead to elevated CVP independent of central circulatory status. Partial compression of the inferior vena cava and transmission of pressure to the thorax can result in high CVP despite relative intravascular hypovolemia. In such situations, CVP provides limited information regarding fluid responsiveness.
Mechanical Ventilation and Elevated Intrathoracic Pressure
During mechanical ventilation, particularly with high positive end-expiratory pressure (PEEP), intrathoracic pressure increases and thereby elevates measured CVP, without necessarily reflecting increased preload. Changes in ventilatory settings may therefore influence CVP independently of true changes in circulatory filling.
Pulmonary Hypertension and Pericardial Conditions
In severe pulmonary hypertension or pericardial conditions with tamponade-like physiology, right-sided pressure dynamics are altered such that CVP primarily reflects afterload and pericardial constraint, rather than volume status or preload responsiveness.
Key Clinical Point
CVP is a pressure measurement, not a measure of volume or cardiac output. In isolated right ventricular failure, significant tricuspid regurgitation, or elevated intra-abdominal pressure, CVP may be high without providing reliable information about preload or fluid responsiveness.
Using SvO₂ and CVP Together – A Practical Model
In clinical practice, these parameters should be used complementarily:
CVP → surrogate for filling pressure and congestion
SvO₂ → surrogate for cardiac output and oxygen balance
The Frank–Starling mechanism still applies, but in heart failure the curve is often:
Flat
Shifted
Highly individual
Therefore, response to interventions is more informative than static values.

Practical Approach When Uncertain: Fluids or Decongestion?
In cardiogenic shock, it is often unclear whether reduced perfusion is caused by insufficient preload or whether the patient is already operating on the flat portion of the Frank–Starling curve with significant congestion. In such situations, static hemodynamic variables alone provide limited decision support. Treatment decisions should therefore be guided by the physiological response to a controlled intervention.
Step 1 – Baseline hemodynamic assessment
The patient presents with:
Low or borderline low central venous oxygen saturation (SvO₂), consistent with low flow
Elevated or difficult-to-interpret CVP
Clinical signs of hypoperfusion
This indicates inadequate oxygen delivery but does not provide definitive information regarding preload responsiveness.
Step 2 – Controlled test intervention
If uncertainty persists, a single controlled intervention is performed, either:
A cautious fluid challenge, or
Unloading (diuretics)
The intervention should be limited, reversible, and followed by early reassessment. The purpose is to reveal the patient’s hemodynamic response, not to deliver definitive therapy.
Note: Inotropic therapy and vasodilation are also key interventions in the management of reduced cardiac output, but these are discussed in detail in another article.
Step 3 – Response-based interpretation
Changes in SvO₂ following the intervention are used as the primary response parameter:
Rising SvO₂ indicates increased cardiac output and supports preload responsiveness
Unchanged or falling SvO₂, particularly if CVP increases simultaneously, indicates lack of preload responsiveness and worsening congestion
The central principle is:
CVP alone is insufficient for decision-making - SvO₂ provides direction.
Clinical implication
This approach enables rational treatment decisions in settings where advanced hemodynamic monitoring is not available. By basing management on physiological response, clinicians can both identify patients who benefit from preload augmentation and avoid further fluid loading in patients in whom it would worsen perfusion.
When SvO₂ Can Be Misleading
SvO₂ can be falsely elevated and mask underlying tissue hypoxia in several situations:
Severe infection, late-phase sepsis or late-phase cardiogenic shock – impaired oxygen utilization
Low oxygen consumption – deep sedation, hypothermia, paralysis
High FiO₂ – acute increase after intubation without perfusion improvement
Arteriovenous shunting – cirrhosis, AV fistulas
Technical issues – sampling errors or catheter malposition
SvO₂ must always be interpreted in the context of Hb, SaO₂, lactate, and clinical findings.
Lactate – A Necessary Corrective Marker
A lactate level > 2 mmol/L is considered consistent with tissue hypoperfusion and is a central criterion in the assessment of shock. In situations where the reliability or interpretability of SvO₂ is uncertain, lactate can provide important complementary information. SvO₂ reflects the instantaneous balance between oxygen delivery and consumption, but may be misleading in conditions with altered oxygen extraction, reduced metabolic demand, or regional maldistribution of flow.
Serial lactate measurements do not provide real-time hemodynamic information, but reflect the cellular consequence of sustained tissue hypoxia. When interpreted together with SvO₂ and the clinical picture, lactate trends can help distinguish true improvement in perfusion from falsely reassuring SvO₂ values.
Rising SvO₂ with falling lactate supports improved global perfusion
Stable or rising lactate despite improving SvO₂ raises concern for ongoing tissue hypoxia or impaired oxygen utilization
Concordant improvement in SvO₂, lactate, and clinical signs strengthens confidence in treatment response
Lactate should therefore be viewed not as an alternative to SvO₂, but as a physiological cross-check, particularly when SvO₂ values are difficult to reconcile with the overall clinical assessment.
When CVP and SvO₂ Are Not Enough
Escalation should be considered when:
SvO₂ remains low or clearly misleading
Clinical findings and hemodynamic data diverge
The patient fails to respond as physiologically expected
In such cases, the threshold for advanced hemodynamic assessment should be low.
Key Clinical Takeaways
Cardiogenic shock is a low-flow shock
Blood pressure alone is misleading
SvO₂ is the most useful real-time flow surrogate
CVP reflects congestion, not volume
Stable Hb and SaO₂ are required for meaningful SvO₂ interpretation
Lactate is a necessary complementary marker
Response to interventions matters more than static numbers
In Brief
In cardiogenic shock, SvO₂ is used to assess cardiac output, while CVP is used to assess congestion. SvO₂ can only be interpreted meaningfully when hemoglobin and arterial oxygen saturation are stable. A rise in CVP without improvement in SvO₂ indicates lack of preload responsiveness and worsening perfusion. Lactate serves as a complementary marker to uncover persistent tissue hypoxia.
Acknowledgement
The author gratefully acknowledges Dr. Eirik Qvigstad for his valuable contributions to this article.
1) What is central venous oxygen saturation (SvO₂)?
Central venous oxygen saturation (SvO₂) reflects how much oxygen remains in the blood after tissue extraction. It represents the balance between oxygen delivery and oxygen consumption and is used clinically as an indirect marker of global circulatory flow.
2) What is the difference between SvO₂ and ScvO₂?
SvO₂ is measured in the pulmonary artery and represents mixed venous blood from the entire body. ScvO₂ is measured via a central venous catheter and reflects venous blood primarily from the upper body. In clinical practice, ScvO₂ is most often available and is used as a trend parameter with awareness of its limitations.
3) When can ScvO₂ be misleading in cardiogenic shock?
In shock states, oxygen extraction and perfusion may be unevenly distributed. In cardiogenic shock, preferential perfusion of the brain and upper body with hypoperfusion of the splanchnic circulation and lower extremities may cause ScvO₂ to overestimate global oxygen balance compared with true mixed SvO₂.
4) When can SvO₂ be used as a surrogate for cardiac output?
SvO₂ can be interpreted as a surrogate for cardiac output when hemoglobin concentration, arterial oxygen saturation (SaO₂), and oxygen consumption are relatively stable. Changes in any of these variables will affect SvO₂ independently of flow.
5) What does a low SvO₂ indicate in cardiogenic shock?
A low SvO₂ in cardiogenic shock usually indicates inadequate oxygen delivery relative to tissue demand, most commonly due to low cardiac output and reduced global circulatory flow.
6) When can SvO₂ be falsely elevated?
SvO₂ may be falsely elevated in conditions with impaired tissue oxygen utilization, such as severe infection or mitochondrial dysfunction, deep sedation, hypothermia, high FiO₂, arteriovenous shunts, or technical sampling errors. In these settings, a high SvO₂ may mask ongoing tissue hypoxia.
7) What is CVP, and what is it used for?
Central venous pressure (CVP) is the pressure in the right atrium and reflects right-sided filling and congestion. CVP is a pressure measurement and does not directly assess volume status or fluid responsiveness.
8) In which situations can CVP be misleading?
CVP may be misleading in isolated right ventricular failure, severe tricuspid regurgitation, portal hypertension with ascites or elevated intra-abdominal pressure, mechanical ventilation with high PEEP, pulmonary hypertension, and pericardial disease. In these conditions, CVP primarily reflects pressure accumulation rather than preload or fluid responsiveness.
9) What does rising CVP without improvement in SvO₂ indicate?
An increase in CVP without a corresponding rise in SvO₂ suggests that the heart is not preload-responsive. Additional filling increases congestion rather than stroke volume, leading to impaired organ perfusion and worsening hemodynamics.
10) How are SvO₂ and CVP used together in clinical practice?
SvO₂ is used as a surrogate for flow, while CVP is used as a marker of congestion. Changes in SvO₂ following a controlled intervention provide more clinically meaningful guidance than isolated CVP values.
11) What is the role of lactate in cardiogenic shock?
Lactate reflects the cellular consequence of sustained tissue hypoxia and has strong prognostic value in cardiogenic shock. While lactate does not provide real-time hemodynamic information, it serves as a physiological cross-check when interpreted alongside SvO₂ and the clinical picture.
12) Is echocardiography used in the assessment of cardiogenic shock?
Yes. Echocardiography is a central component of hemodynamic assessment in cardiogenic shock and can identify underlying mechanisms such as left or right ventricular failure, valvular disease, and pericardial pathology.
13) Can echocardiography be used to estimate cardiac output?
Yes. With adequate imaging quality, accurate measurement of the left ventricular outflow tract (LVOT), and a representative LVOT VTI signal, cardiac output can be reliably estimated. This article nevertheless focuses on CVP and SvO₂ as continuously available surrogate parameters.
14) Are CVP and SvO₂ sufficient to guide treatment in cardiogenic shock?
No. CVP and SvO₂ are useful tools, but management of cardiogenic shock must always be based on an integrated assessment incorporating clinical findings, echocardiography, laboratory data, and response to therapy.



Comments